
What Is Positional Sleep Apnea?
For many people with obstructive sleep apnea (OSA), breathing events do not happen evenly across all sleep positions. Apneas tend to be more frequent, and more severe, when sleeping on the back. When the airway is significantly worse on the back than on the side, this is called positional OSA.
The most widely used research definition is the Cartwright criterion. Positional OSA is present when the supine apnea-hypopnea index (AHI) is at least twice the non-supine AHI. By that definition, roughly half of all people with OSA are positional. A smaller group has exclusively positional OSA — meaning the non-supine AHI is in the normal range (under 5 events per hour).
If your sleep study report breaks out events by body position, look for a "supine AHI" line and a "non-supine AHI" line. A wide gap between the two is the signal that positional therapy may help you.
Why Position Matters
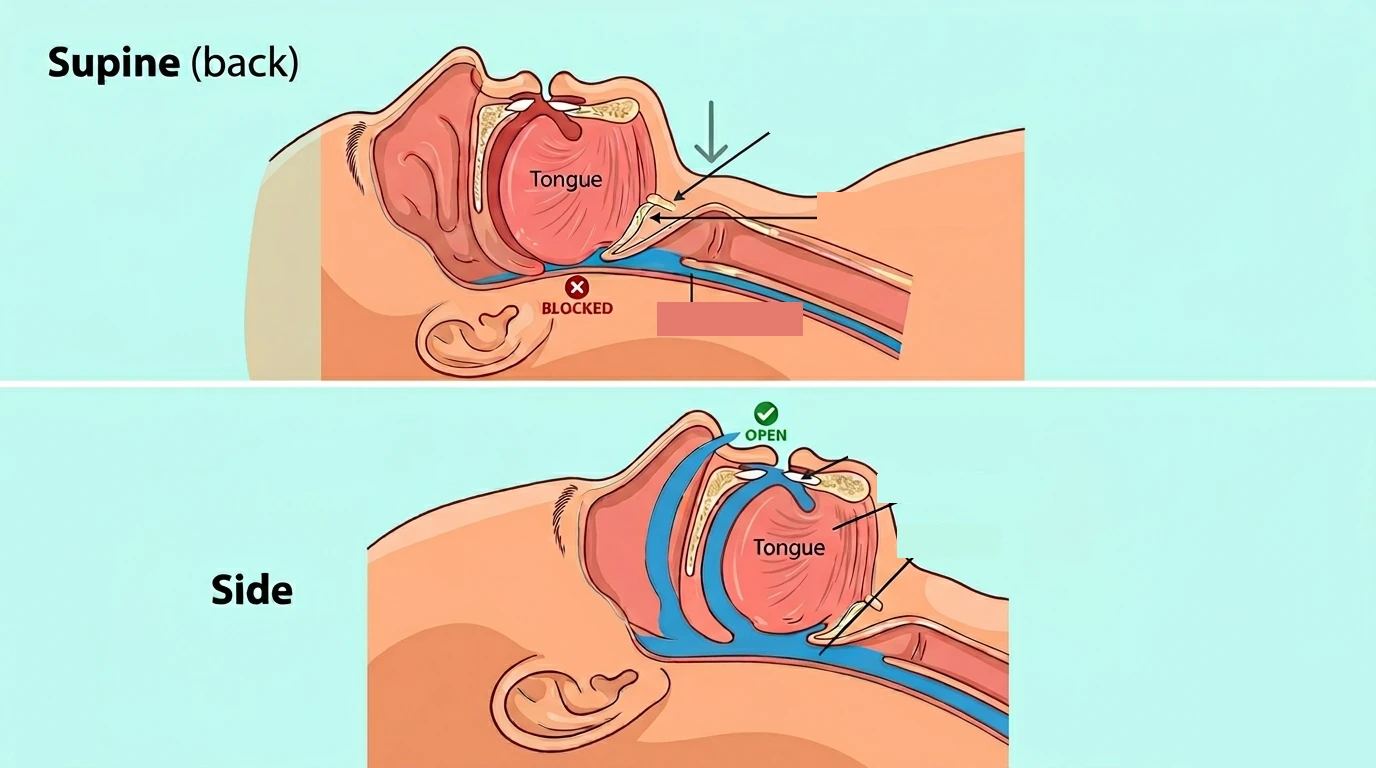
When you lie on your back, gravity pulls the tongue and the soft tissues of the throat downward toward the back of the airway. The lower jaw also tends to fall back. These shifts narrow the upper airway at exactly the moment muscle tone is lowest — during sleep. On the side, the tongue and soft palate are no longer fighting gravity in the same way, and the airway tends to stay open.
This is why bed partners often notice that snoring and gasping events get loud once the sleeper rolls onto their back, then quiet down again on the side.
Who Is a Candidate?
Positional therapy is most useful when:
- A diagnostic sleep study has shown positional OSA (supine AHI at least twice the non-supine AHI)
- The non-supine AHI is mild or normal
- You currently spend a meaningful percentage of the night on your back
- You have not tolerated CPAP, or you are looking for an additional treatment to reduce residual events
It is not a stand-alone treatment for severe OSA, severe oxygen desaturation, or apnea that persists in every body position. People who already sleep almost entirely on their side and still have a high overall AHI are not good candidates either, because position is not the main driver of their breathing events.
This decision should be made with your sleep physician, ideally with the position-specific data from your sleep study in hand.
How Effective Is It?
When positional therapy successfully keeps a person off their back, randomized trials and meta-analyses tend to show:
- A drop in overall AHI, often into the mild or normal range for the right candidates
- A reduction in supine sleep time — typically from 30–50 percent of the night down to under 5 percent
- Less snoring and fewer oxygen desaturation events
- Outcomes that approach — but do not consistently match — CPAP for moderate OSA
Long-term adherence is the main factor that decides whether positional therapy actually works for a given patient. Older approaches like the tennis-ball-in-a-shirt technique often disturb sleep and end up abandoned within a few weeks. Vibrotactile devices were designed to address that problem, and their long-term use rates in published studies are noticeably higher than belt or bulk methods.
Devices and Approaches

Product images courtesy of Night Shift Therapy, Zzoma, K2 Health Products, and Positional Sleep Systems. Used for editorial reference.
Vibrotactile Position Trainers
These devices sense when you have rolled onto your back and produce a gentle vibration. The vibration prompts you to roll without fully waking you. They do not block back-sleeping with bulk; they retrain the behavior. Six-month adherence rates of around 70 percent have been reported, well above what older methods achieve.
- Night Shift by Advanced Brain Monitoring is a small, FDA-cleared device worn on the back of the neck like a soft collar. It vibrates with progressively stronger pulses when you roll supine, and it records position, snoring loudness, and sleep quality data that you can download.
- Philips NightBalance / Lunoa is a chest-worn vibrotactile trainer that has been studied widely in positional therapy trials. Availability has changed in some regions, so check current distributor status before ordering.
- Somnibel is a small adhesive sensor worn on the forehead that delivers vibratory feedback when you turn supine. It is used in several European clinical studies.
When shopping for any of these devices, current availability and pricing change often, so check the manufacturer's site directly and confirm with your sleep clinician that the device you are considering fits your situation.
Belts and Bumper Devices
These work by making the supine position physically uncomfortable. They are simpler and less expensive than vibrotactile trainers, but adherence over months tends to be lower because the bulk can disturb sleep.
- Zzoma Positional Device is an FDA-cleared semi-rigid foam belt worn around the chest with a bumper at the back. It was designed for positional OSA and studied in peer-reviewed trials.
- Sleep Noodle (CPAPology) is a breathable belt with a long foam noodle that sits across the upper back, training the wearer to stay on their side.
- The bumper belt or "tennis ball shirt" is the do-it-yourself version: a sock or pouch holding one or more tennis balls sewn into the back of a snug t-shirt. It is cheap and easy to try as a proof of concept, but most people find it uncomfortable for long-term use.
Pillows and Wedges
- Contoured anti-snoring pillows are shaped to encourage side sleeping with the head and neck positioned to keep the airway open. Several FDA-cleared options are available.
- Side-sleep back pillows are firm cushions or body pillows placed behind a side-sleeper to physically block rolling onto the back. Designs range from simple bolster shapes to curved pillows that also support the head (one example is sold at positionalsleep.com). A long generic body pillow set behind the back works for many people.
- Wedge pillows or head-of-bed elevation. Sleeping with the upper body elevated 30 to 45 degrees can reduce supine apnea events on its own. A bed wedge or an adjustable bed frame achieves this. It is most useful as an addition to other treatment, especially when reflux or nasal congestion are also part of the picture.
Combining Positional Therapy With Other Treatments
Positional therapy is increasingly used alongside other treatments rather than instead of them.
People using a mandibular advancement device often have residual supine events. Adding a position trainer can close that gap. Some patients on CPAP can also tolerate a lower pressure once they consistently sleep off their back, which improves comfort and adherence. After upper airway surgery, including hypoglossal nerve stimulation, residual events that are concentrated on the back can sometimes be addressed with positional therapy as well.
Practical Tips for Success
- Use the device every night for the first 4 weeks, including for naps. The behavioral retraining effect is strongest in the first month.
- Treat nasal congestion. Side sleeping does not help much if you cannot breathe through your nose. Saline rinses, nasal steroid sprays (with your doctor's input), and treating any underlying allergies all support the therapy.
- Avoid alcohol within 3 hours of bed. Alcohol relaxes throat muscles and disproportionately worsens supine OSA.
- Re-test after 4–8 weeks of consistent use. Ask your sleep clinician about a follow-up home sleep test or a data download from a recording device — the Night Shift produces its own reports, for example. Objective evidence that the overall AHI has dropped is more reliable than how you feel.
- Do not stop CPAP without confirmation. If you are considering a switch from CPAP to positional therapy, document the change in AHI with testing first. Feeling rested is not always a reliable signal in OSA.
When Positional Therapy Is Not Enough
If a follow-up study shows that your overall AHI is still elevated despite consistent off-back sleep, position was not the main driver and another treatment is needed. Common signs include:
- A non-supine AHI in the moderate-to-severe range
- Significant oxygen desaturations regardless of position
- Daytime sleepiness or cardiovascular risk factors that have not improved
In those cases, CPAP (our CPAP Setup Guide covers getting started), an oral appliance, or surgical options (including hypoglossal nerve stimulation for selected patients) should be revisited with your sleep physician.
Key Takeaways
- Positional OSA — defined as supine AHI at least twice the non-supine AHI — is present in about half of OSA cases.
- Vibrotactile position trainers (Night Shift, Philips NightBalance / Lunoa, Somnibel) have substantially better long-term adherence than older tennis-ball methods.
- Belts (Zzoma, Sleep Noodle), back-blocking side-sleep pillows, and wedge pillows are simpler, lower-cost options to consider.
- Positional therapy works best for the right candidates with mild positional OSA, or as an addition to CPAP or oral appliances for others.
- Any switch in therapy should be confirmed with objective testing rather than how you feel.